See a Demo
You're just one step away from seeing Call Loop in action.
Enter your information below to watch a demo right now.
You're just one step away from seeing Call Loop in action.
Enter your information below to watch a demo right now.

A missed appointment isn't just an empty slot on the schedule. It’s clinician time that can’t be recovered, staff effort that produced no care, and a patient who may now be further from diagnosis, treatment, or follow-up.
The useful shift is this: no-shows are not random. They usually come from a small set of operational failures that practices can identify and fix. In 2025, 73% of medical practices reported patient no-show rates either stayed the same or decreased, and they largely credited consistent communication strategies such as digital reminders, automated calls, and occasional live outreach according to the MGMA Stat poll on patient no-shows in 2025.
That matters because it reframes how to reduce patient no shows. The answer is rarely a single reminder text. The practices that make progress usually combine scheduling access, clear cancellation rules, easy rescheduling, and a multi-channel reminder process that reaches patients the way they respond.
One no-show rarely stays contained to one no-show.
A new patient misses an intake. The provider loses a high-value slot. The front desk has a gap they can’t fill on short notice. A referral source waits longer for feedback. The patient often doesn’t disappear either. They call back later, usually needing another prime appointment time, which pushes someone else further out.
That’s the operational cost. The clinical cost can be worse.
When patients miss follow-up visits, medication checks, prep-dependent procedures, or chronic care reviews, practices don’t just lose productivity. They lose continuity. Staff then spend time chasing the patient, documenting outreach, re-verifying coverage, and rebuilding a visit that should have happened the first time.
The mistake many practices make is treating no-shows as a patient discipline issue. Some no-shows are about forgetfulness, but many come from friction the practice created without meaning to. Long lead times, confusing instructions, weak reminder workflows, hard-to-reach scheduling teams, and cancellation processes that feel like work all push patients toward silence instead of communication.
Practical rule: If a patient can’t confirm, ask a question, or reschedule in under a minute, your reminder process is incomplete.
The good news is that most no-show reduction work is operational, not mysterious. Practices that improve usually do a few basic things consistently. They shorten the time between booking and visit. They make reminders conversational instead of one-way. They stop relying on one channel. And they remove avoidable barriers before the appointment becomes a missed appointment.
That’s where the return sits. Not in punishing absence after the fact, but in designing a system that makes attendance easier than disappearing.
Practices with high no-show rates rarely have one attendance problem. They usually have three or four smaller problems hiding inside the schedule.

That is why the first job is diagnosis. Pull the data from your EHR or practice management system and identify where missed appointments cluster. In real practices, the pattern often shows up around new patient visits, prep-heavy procedures, long-booked follow-ups, Monday mornings, or one provider whose schedule runs further out than everyone else.
A no-show problem has a shape. If you miss that shape, you end up sending the same text reminder to every patient and wondering why results stay flat.
Use one formula and stick to it: (no-shows / total appointments) x 100.
That sounds basic, but I see teams derail here all the time. Front desk may count only true no-shows. Operations may include late cancellations that could not be refilled. Billing may look at something else entirely. If each department is tracking a different numerator, no one can tell whether the problem is getting better or worse.
Pull at least these views:
That last field is where many practices find the operational gap.
Counts matter, but patterns matter more. A schedule full of misses six weeks out calls for a different response than a schedule full of missed colonoscopy consults or behavioral health follow-ups.
Use a simple pattern review like this:
| Pattern you see | Likely cause |
|---|---|
| More misses on visits booked far in advance | Long lead time, lower urgency, higher life disruption risk |
| More misses on prep-heavy visits | Instructions unclear, anxiety, or prep not understood |
| More misses in specific neighborhoods | Transportation friction or inconsistent phone service |
| More misses among certain patient groups | Communication channel mismatch |
| More misses after eligibility or estimate discussions | Financial hesitation |
Channel strategy transitions from theoretical to practical. If text messages are delivered but older patients respond to voice, or if mobile numbers are outdated in a rural population, an SMS-only workflow leaves money on the table. Practices usually do better with a HIPAA-safe reminder system that can mix text, email, live-call escalation, ringless voicemail, and voice broadcasting based on patient behavior. This guide to HIPAA-compliant appointment reminder workflows covers the communication side in more detail.
Review the process step by step, from scheduling to appointment time.
Ask direct questions:
Weakness in any of those steps creates avoidable misses. The reminder may have gone out. The patient still may not have had a usable path to respond.
I also recommend reviewing your attendance policy against a clear external model such as the Insight Diagnostics DNA policy. The value is not copying another clinic word for word. The value is seeing whether your own process clearly defines reminders, patient responsibility, documentation, follow-up, and escalation after repeated absences.
One more point often gets missed. Contact data quality is part of no-show analysis. If numbers are outdated, consent records are incomplete, or patients were never asked for their preferred channel, your communication performance report will look better than the patient experience. Delivery is not the same as reach.
The practices that reduce no-shows fastest are usually the ones that stop treating every empty chair as the same event. They identify which appointments are at risk, which patients need a different channel, and where staff workflow is creating friction. That is how a vague attendance problem becomes a set of fixable operational issues.
Practices that cut no-shows usually fix access and policy before they add more reminders. If the appointment is booked too far out, the cancellation path is clumsy, or staff apply rules inconsistently, missed visits stay high no matter how many texts go out.
A no-show resistant schedule starts with fewer opportunities for patients to fall off the calendar. That means shorter lead times, clear attendance expectations, and booking rules based on actual demand patterns.
Long booking windows create failure points. Transportation changes. Work schedules shift. Symptoms improve. Patients forget why they booked in the first place.
Research published in PMC on open access scheduling found lower no-show rates, shorter appointment delays, and better patient satisfaction when practices reduced wait times and expanded same-day access. The operational lesson is straightforward. The longer the gap between booking and visit, the more likely life gets in the way.
Start by reviewing how many appointments sit weeks out that could be handled sooner. Follow-ups are often the easiest place to intervene. In primary care and many specialty groups, holding back some same-day or next-day capacity improves attendance without adding staff.
A few scheduling changes usually produce the fastest return:
A policy fails when the patient understands it but cannot act on it.
I see this often. The practice asks for 24 hours' notice, but the only way to cancel is to call during office hours, wait on hold, and hope someone answers. Patients who hit that friction late in the day often do nothing. The result is a silent no-show that could have become a refillable opening.
Easy rescheduling should be built into the policy itself. Patients need a clear way to confirm, cancel, or request a new time without starting from zero. That is one reason multi-channel outreach works better than SMS alone. Some patients will tap a text link. Others will respond to a call, a voicemail drop, or a live outreach attempt after they miss earlier messages.
A good attendance policy is easy to read, easy for staff to explain, and easy for patients to follow.
For practices reviewing how others formalize attendance expectations, the Insight Diagnostics DNA policy is a useful example of how to set expectations in writing without making the policy feel hostile.
Patient agreements can help in the right cases. They are most useful for repeat no-show patients, high-demand consults, imaging, procedures, and any visit where prep time or reserved resources create real cost.
The wording matters. A blunt agreement can damage trust and increase friction at the front desk. A clear agreement sets mutual expectations. It explains what the practice will do, what the patient needs to do, and what happens after repeated missed appointments.
Useful elements often include:
Staff need a script, not just a form. If each scheduler explains the policy differently, enforcement gets uneven and patients push back.
Overbooking should be precise. Broad double-booking is usually a sign that the schedule template is masking a deeper access problem.
Use your own history to identify where no-shows cluster by provider, appointment type, day of week, or time of day. Then test limited overbooking only in those segments. A cardiology group might find that low-acuity follow-ups on Friday afternoons have enough fallout to justify one extra slot. A surgical clinic with long room times and prep requirements usually cannot absorb that risk without creating delays.
The trade-off is simple. An empty chair wastes capacity. A full waiting room burns patient goodwill and staff time.
A practical rule is to overbook only where your data supports it and where the provider can absorb variation without running behind all session.
Fees, deposits, and card-on-file policies can reduce avoidable misses, but they should be used selectively. They work better for high-demand specialties, procedure-based care, and patients with repeated no-shows than they do for routine visits where price sensitivity is high.
Practices need to weigh deterrence against access. A strict no-show fee may improve attendance in one segment while causing other patients to avoid booking at all. That is a poor trade if the practice serves cost-sensitive populations or relies on long-term continuity.
If you use fees or deposits, keep the policy operationally clean:
Communication and policy have to match. If patients can confirm by text but cannot cancel except by phone, staff will still lose appointments they could have saved. Practices building those workflows can use this HIPAA-compliant appointment reminder guide as an operational reference for aligning consent, channel rules, and response handling.
Good policy reduces friction before the reminder sequence begins. That gives your multi-channel outreach a better chance to fill the slot instead of documenting the miss.
Most reminder systems fail for one reason. They assume one message on one channel is enough.
It usually isn’t.
A patient may ignore texts at work, miss phone calls from unknown numbers, and never check email. Another may prefer a call because they’re older, rural, or less comfortable with portals and links. A strong system doesn’t force one behavior. It uses SMS, voice broadcasting, and ringless voicemail together, with two-way response options and clear pathways to confirm or reschedule.
According to the Qminder guidance on reducing no-show rates, a multi-channel automated reminder system can reduce no-shows by up to 40%, phone reminders cut no-shows from 23% to 13%, and 73% of successful practices use two-way communication. That last point is the one many teams miss. One-way reminders notify. Two-way reminders solve problems before the slot is lost.
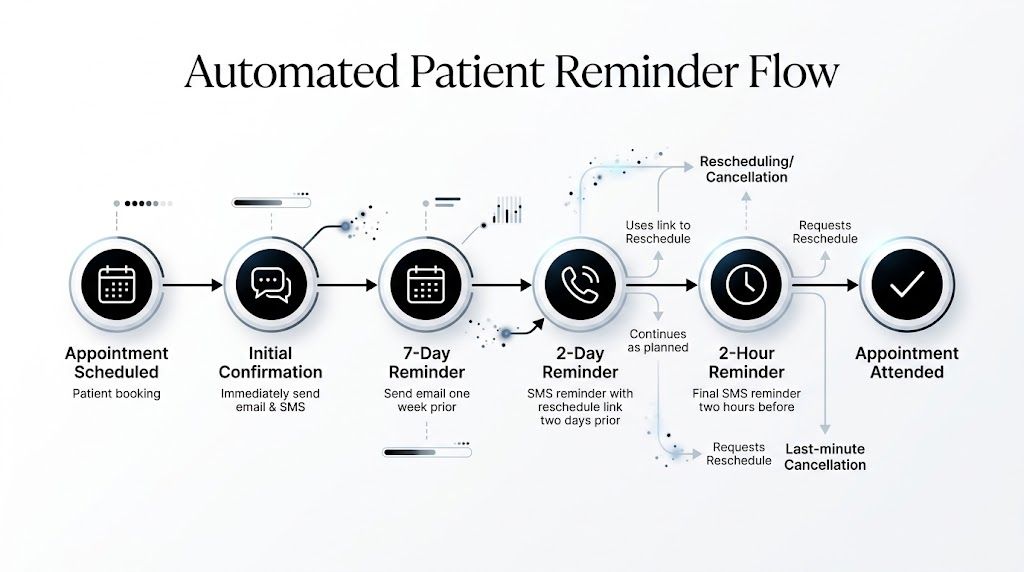
The sequence matters as much as the wording.
Each touchpoint should have a job. One confirms the appointment exists. Another gives enough notice to rearrange life. Another captures late friction and prompts action. If there’s still silence, the system should escalate the channel or route the patient to staff.
Here’s a practical framework.
| Timing | Channel | Message Content / Goal |
|---|---|---|
| At booking | SMS or email | Confirm date, time, location, and next step. Catch bad contact info immediately. |
| 7 days before | SMS or voice | Early reminder. Invite confirmation or rescheduling while options still exist. |
| 48 hours before | SMS with two-way reply | Ask patient to confirm, ask a question, or tap to reschedule. |
| 24 hours before | Voice call or ringless voicemail for non-responders | Reach patients who ignore text. Reinforce attendance details and response options. |
| Day of visit | Short SMS | Final prompt with arrival or check-in detail. |
| After missed confirmation | Automated follow-up | Offer reschedule path instead of waiting for a no-show. |
That framework is adaptable. A prep-heavy procedure may need more education earlier. A routine follow-up may need less language and more simplicity.
Text is fast, direct, and easy for most patients. But many practices waste it on passive messages.
A better SMS reminder does three things:
Examples:
SMS example
Dr. Lee’s office: You’re scheduled for Tuesday at 10:30 AM. Reply C to confirm or R to reschedule.
SMS example
Reminder from Valley Clinic. Your appointment is tomorrow at 2:00 PM. Need to change it? Reply R and we’ll send options.
The goal isn’t to cram every detail into one message. The goal is to prompt a decision.
If a patient doesn’t respond, that’s useful signal. It tells you who needs a second channel.
Healthcare teams sometimes treat voice as outdated. That’s a mistake.
Voice remains effective for older patients, patients with lower digital comfort, patients with prep anxiety, and visits where details matter. Automated voice broadcasting is also useful when you need consistency across a large schedule but still want a more human-feeling reminder.
A strong voice reminder includes:
If your platform supports AI text-to-speech, staff can standardize messaging without recording fresh audio for every update. If it supports press-1 transfers or similar routing, patients can move directly into a reschedule or question workflow.
For practices comparing workflow options beyond healthcare-specific tools, it can help to understand call centre software features and pricing because features like call routing, queue handling, and answer detection affect how reminder escalations perform in practice.
This is the underused channel most practices should at least test.
Ringless voicemail delivers a voice message directly to the patient’s voicemail inbox without requiring a live answer. That makes it useful when patients ignore unknown calls, don’t respond to texts, or prefer listening over reading. It’s particularly practical for elderly patients, low-tech populations, and patients who never engage with links.
The value of ringless voicemail is not novelty. It’s coverage.
A patient may not answer a standard call from a clinic number they don’t recognize. They may not open a text if they’re busy. But they may listen to a voicemail while driving home, during a break, or when reviewing missed messages. For reminder workflows, that creates a useful middle ground between intrusive calling and passive texting.
A simple ringless voicemail script works best:
This is a reminder from Lakeside Medical. You have an appointment on Thursday at 9:00 AM. If you need to reschedule, please call us or use the link sent to your phone. We look forward to seeing you.
Keep it short. Use plain language. Mention the action. Don’t bury the purpose.
A reminder engine should not treat every patient the same.
Segment by factors you already have:
For example, a new patient with a history of non-response may get SMS plus voice plus ringless voicemail. A reliable returning patient may only need one two-way text. A rural patient who rarely clicks links may do better with voice and a simple callback option than with SMS alone.
This is also the right point to mention tools. A platform such as Call Loop’s automated appointment reminder workflow can coordinate SMS, voice broadcasting, and ringless voicemail in timed sequences with segmentation, scheduling, merge tags, and analytics. That kind of orchestration is what makes multi-channel practical instead of manual.
Even good reminder systems break in predictable ways.
Here are the ones I see most often:
The reminder that matters most is the one that gives the patient an easier alternative than not showing up.
Reminder copy often sounds like it was written for compliance review instead of human use. Keep messages clear, respectful, and short.
Good reminder language is:
Bad reminder language is packed with policy wording, abbreviations, and unnecessary detail.
For prep-dependent appointments, add only the critical instruction and point to the full details elsewhere. For example, remind the patient there is preparation required and how to get help if they’re unsure. If the prep is confusing, people disappear rather than admit they don’t understand.
The strongest reminder engine doesn’t rely on one heroic message. It uses a timed sequence, channel escalation, patient preference, and an easy response path so attendance becomes the simplest option.
A reminder system isn’t finished when it goes live. It’s finished when it produces stable attendance patterns month after month.
The first mistake practices make is tracking only the final no-show rate. That tells you the outcome, but not where the system is breaking. If your no-show rate is unchanged, you need to know whether messages weren’t delivered, weren’t read, weren’t acted on, or reached the wrong patients on the wrong channel.
Watch metrics that show movement before the appointment is lost:
That’s where segmentation starts to matter.
The Alliance resource points to an underserved opportunity in tailoring reminders for higher-risk groups. It notes that calendar invites can reduce no-shows by up to 25% for certain groups, and AI-powered segmentation can reduce no-shows by 10% to 15% for every week of shortened lead-time, as discussed in the Alliance best-practices tip sheet for reducing patient no-shows.
Don’t rewrite your full workflow every month. Change one variable, observe it, and keep what improves patient response.
Test things like:
| Variable | What to test |
|---|---|
| Channel order | SMS first, then voice, versus voice first for older cohorts |
| Message style | Short directive copy versus warmer conversational copy |
| Timing | Earlier reminder for specialty visits versus tighter timing for primary care |
| Response path | Reply keyword, callback number, or direct reschedule link |
| Segment rule | Separate workflows for new patients, procedures, and repeat no-show patients |
This is the same discipline marketers use when improving conversion paths. If your team wants a simple framework for structured testing, Gorilla's conversion optimization insights offer a useful way to think about small changes that compound.
Analytics are only useful if someone owns the next step.
If older patients confirm more often through voice than text, update the preference rule. If one provider’s Friday schedule has chronic non-response, adjust booking patterns. If prep-heavy visits show high non-response at the 48-hour mark, trigger live outreach sooner.
For teams already using campaign dashboards, the same measurement logic applies to reminders. The framework for measuring campaign effectiveness is useful because it pushes teams to connect message delivery, engagement, and outcomes rather than staring at one top-line number.
Better no-show performance usually comes from better segmentation, not louder reminders.
Practices that keep improving don’t assume all patients behave alike. They tighten lead times where possible, learn which channel works for which patient, and treat every non-response pattern as a clue rather than a dead end.
No. A fee can help in the right context, but it shouldn’t be the first tool you reach for.
For high-demand consults, expensive prep, or repeat offenders, a fee or deposit may be reasonable if the rule is clear and consistently explained in advance. For general care, using fees as the main strategy often backfires. Patients who are already anxious about cost may avoid rescheduling and disappear. In most practices, access, communication, and reminder design produce cleaner results than punishment alone.
Treat chronic no-shows as a workflow segment, not just a behavior problem.
Give them a tighter scheduling model. Offer same-day or short-lead appointments where possible. Use stronger confirmation rules. Route them into a higher-touch reminder sequence. If the patient repeatedly misses despite support, then apply a documented attendance policy and rebooking conditions. The goal is to protect capacity without making staff negotiate the rules from scratch every time.
Often, no.
Text works well for many patients, but not all of them. Some patients don’t respond to links, some ignore unknown messages, and some are much more likely to listen than read. That’s why practices trying to learn how to reduce patient no shows effectively should think in layers, not channels. SMS is one layer. Voice is another. Easy rescheduling is another. Staff escalation for high-risk visits is another.
Ringless voicemail is useful when patients ignore texts or don’t answer calls, but still listen to voicemail messages later. The Kyruus resource notes that ringless voicemail is an under-explored, HIPAA-compliant tool that can help reach non-digital-preferring patients such as the elderly, as explained in Kyruus Health’s discussion of negating patient no-shows.
That makes it practical for:
It’s not a replacement for SMS. It’s a complementary channel that fills a gap.
More than most practices do now.
At minimum, personalize by appointment type, patient preference, language, and no-show risk. A routine follow-up doesn’t need the same sequence as a new patient consult or a procedure with prep. Patients with transport or financial barriers may need more than a reminder. They may need earlier outreach, a chance to reschedule easily, or staff intervention before the day of service.
Three things.
First, the data is wrong. Old phone numbers and weak intake validation will sink automation fast. Second, the reminder is one-way, so patients who need help have no simple next step. Third, the sequence stops at “message sent” rather than “patient responded.” Good systems don’t just send reminders. They create movement toward confirmation, cancellation, or rescheduling.
If your practice wants a practical way to run HIPAA-compliant reminders across SMS, voice broadcasting, and ringless voicemail without stitching together manual workflows, Call Loop gives teams a way to build timed sequences, segment patients, and automate confirmations and rescheduling outreach across the channels patients respond to.
Chris Brisson
Chris is the co-founder and CEO at Call Loop. He is focused on marketing automation, growth hacker strategies, and creating duplicatable systems for growing a remote and bootstrapped company. Chat with him on X at @chrisbrisson
Trusted by over 45,000 people, organizations, and businesses like






